

H.O.P.E. Re-connect Form
Hope Opportunity Prosperity through Education Needs Assessment

At Fayetteville Technical Community College (FTCC), we recognize the National Association of Credential Evaluation Services (NACES) as an accredited and trusted provider of credential evaluation services. NACES is a reputable association of U.S.-based, independent, non-governmental organizations that evaluate academic credentials earned outside the United States.
We welcome international and foreign students to apply to our programs, and we are committed to ensuring a smooth and thorough process for evaluating your credentials. If you are an international student, please have your academic documents evaluated by a NACES member organization to confirm their U.S. equivalency. This step is essential to ensure your eligibility for admission to our programs.
FTCC is excited to support students from all over the world and looks forward to your application!
For additional information, click on the button below to view the current members of NACES.
Click on a tile below to learn more!


![]()
Karen Adamson, M.Ed.
Instructional Coach
VCC 201
(910) 486-7408
adamsonk@faytechcc.edu
Karen Adamson is an Instructional Coach at Fayetteville Technical Community College a constituent of the North Carolina Community College System. She brings 17 years’ experience as an Instructional Coach, mentor and teacher. Ms. Adamson holds a Masters of Education degree in Educational Leadership from Concordia University at Portland. She is a proud graduate of Fayetteville State University where she received a Bachelor’s of Art degree in English Language and Literature with a minor in Sociology. Karen is also certified and licensed by the North Carolina Department of Public Instruction. An experienced Professional Development (PD) leader, Karen has created and facilitated PD as Lead Mentor for Beginning Teachers Cohorts seeking licensure in our state, both online and face-to-face.
A life-long resident and product of Cumberland County Schools, Karen is a graduate of Westover Senior High School. Active in ministry, Karen may be found on Clubhouse Platforms and on Facebook. As a writer, editor, poet and spoken word artist, Karen may be also found performing in various venues and poetry events in the city. Karen is also the mother of four children Jordan, Aaron, Aaliyah and Jaedon, as well as the grandmother of five beautiful grandchildren.

![]()
Dr. Andrea Jackson
Coordinator of the Center for Faculty Development
VCC 206
(910) 678-8415
jacksonac@faytechcc.edu
Andrea has worked in the field of education for over 20 years. She has been a resident of Fayetteville for quite some time and is an alumnus of Fayetteville State University. Andrea previously enjoyed a career in cosmetology, prior to entering the field of education. She is very active in the community as a member of her sorority. She is also the mother of 3 wonderful adult children.
Andrea holds a B.A. in English Literature from Fayetteville State University, an M.Ed. in Reading (K-12) from Benedictine University, an M.Ed. in Educational Leadership from Concordia University, an Ed.S. in Educational Leadership from Nova Southeastern University, and an Ed.D. in Instructional Leadership from Northcentral University.
As the Coordinator/Instructional Coach here at FTCC, Andrea’s goals are to utilize her strong knowledge of current trends and best practices in education to support instruction and learning. She believes everyone has a task in life and we should each spend time daily fulfilling that task.

Ken Buckey, Ed.D.
CFD Fellow/Quality Assurance
Department Chair for Emergency Management and Fire Protection
(910) 678-0046
buckeyk@faytechcc.edu
Dr. Ken Buckey serves as the Department Chair for Emergency Management and Fire Protection at Fayetteville Technical Community College in North Carolina. With a decade of experience teaching at the collegiate level, both online and face-to-face, Dr. Buckey has a strong passion for education and is committed to sharing his knowledge while gaining new insights from his students. The majority of his teaching has been in online settings, where he has developed a keen understanding of the unique challenges and opportunities in digital education.
Recently, Dr. Buckey embarked on Quality Matters (QM) reviews, where he has gained valuable insights into maintaining and enhancing the content and quality of his courses. His dedication to continuous improvement is further demonstrated by his extensive training in faculty development, course mapping, and instructional design. Over the years, he has built a broad and deep knowledge base that he is eager to share with his colleagues, helping to ensure that courses across the college meet the highest standards of quality.
Dr. Buckey holds a Master of Science in Management and Homeland Security and a Doctorate in Educational Leadership from Wingate University. His combination of academic expertise and practical experience positions him as a crucial asset to FTCC, where he is committed to supporting fellow instructors in course design, ensuring that both content and delivery are aligned with best practices in education.

Elisa Hill, B.S., RT-RM
CFD Fellow/Educational Technology Support
Radiography Clinical Coordinator and Instructor
(910) 678-9867
hille@faytechcc.edu
Elisa Hill, a native of Fayetteville, NC, and proud graduate of Reid Ross Senior High School, has dedicated her career to the field of Radiography. After completing her education at Fayetteville Technical Community College (FTCC) in 1986, Elisa embarked on a 23-year tenure at Cape Fear Valley Medical Center, where she excelled in various roles including Diagnostic Technologist, OR Technologist, CT Technologist, Lead Technologist, and Radiography Clinical Instructor.
In addition to her full-time work at Cape Fear, Elisa also served as a part-time adjunct clinical instructor at FTCC for five years, transitioning to a full-time role in 2010. Initially a Radiography instructor, Elisa took on the role of Radiography Clinical Coordinator and Instructor in 2020. Her passion for education extends beyond delivering content; she is deeply committed to inspiring and empowering her students and new faculty members alike.
Elisa holds an Associate in Applied Science from FTCC and a Bachelor of Science from Campbell University, earned in 2017. As a seasoned mentor, she has played a crucial role in helping new faculty members navigate platforms like Blackboard, enhancing their teaching capabilities in Allied Health.
Elisa has been married for 31 years and is the proud mother of 26-year-old twins. She looks forward to continuing to share her knowledge and experience with her colleagues at FTCC.

Michelle Robinson, M.S.
CFD Fellow/Innovative Resources
Mathematics Instructor
(910) 678-0060
robinsom@faytechcc.edu
Michelle Robinson is a highly skilled Mathematics Instructor with over 25 years of experience in diverse educational settings. A proud graduate of Fayetteville State University, she holds both a Bachelor of Science in Mathematics Teaching (Cum Laude) and a Master of Science in Mathematics. Her extensive teaching career at Fayetteville Technical Community College (FTCC) began in 2005, where she has since become a cornerstone of the Mathematics Department.
Throughout her career, Michelle has been dedicated to breaking down complex mathematical concepts, making them accessible and understandable for students. Her creative use of instructional materials has consistently increased student engagement and success, both in face-to-face and online environments. She has a strong history of developing innovative lesson plans, integrating technology, and fostering a growth mindset among her students.
At FTCC, Michelle serves as the Coordinator of Proctored Testing in the Math Department’s Computer Lab, where she has created and managed systems that enhance the testing experience and provide a calming environment conducive to student success. Her teaching repertoire includes courses ranging from developmental mathematics to college-level subjects like Quantitative Literacy, Financial Literacy, and Calculus.
In addition to her instructional role, Michelle has a significant impact on curriculum development and instructional design. She has designed and constructed mathematics courses in Blackboard, ensuring a consistent and effective workflow for students. Her commitment to student success is further demonstrated through her weekly check-ins, which address both academic and emotional needs.
Michelle’s contributions to the field of education extend beyond the classroom. She has served as a speaker at the National Youth at Risk Conference, mentored students individually to enhance their math skills, and led the High School Mathematics Department as Head during her tenure at Cumberland County Schools. Her professional development is ongoing, with certifications in Quality Matters, Microsoft Office, and digital literacy, as well as active participation in Pearson’s Digital Advisory Community.
Recognized for her excellence in teaching, Michelle was a recipient of the League of Excellence Award for 2022-2023. She continues to bring her wealth of knowledge and passion for mathematics to FTCC, where she is committed to fostering an inclusive and supportive learning environment that empowers students to achieve their academic goals.

CFD Fellow/Instructional Strategies/Methods
Communications Instructor
LRC 121
(910) 678-9842
kellys@faytechcc.edu
Dr. Sonny Kelly, a dynamic professional with a rich background in performance, storytelling, motivation, and scholarship, brings his multifaceted expertise to the role of Faculty Fellow at FTCC’s Center for Faculty Development.
Currently serving as a full-time professor of Communication, specializing in Public Speaking and Interpersonal/Intercultural Communication, at Fayetteville Technical Community College, Dr. Kelly is an accomplished scholar with a Ph.D. in Communication and Performance Studies from UNC Chapel Hill. He also holds a Master’s degree in Communication Studies from St. Mary’s University and a Bachelor’s degree in International Relations from Stanford University.
For over two decades, Dr. Kelly has captivated audiences nationwide as a storyteller, actor, motivator, lecturer, and trainer. He is the visionary founder and CEO of Legacy Heirs Productions, Inc., a company dedicated to crafting and sharing inspirational and motivational performances and art.
As a Faculty Fellow, Dr. Kelly will contribute his wealth of knowledge and creativity to initiatives aimed at educating, engaging, and empowering diverse audiences across the globe. His unique blend of communication, performance, and scholarship will undoubtedly make a profound impact on the faculty development efforts at FTCC.

CFD Fellow/Instructional Design
Radiography Instructor
HTC 169-G
(910) 678-0153
hoefline@faytechcc.edu
Born in Oklahoma and raised in Fayetteville, Eunice Hoefling has deep roots in the community. Graduating early from Terry Sanford High School, she embarked on a journey of lifelong learning right in the heart of Fayetteville at Fayetteville Technical Community College (FTCC). In 1997, Eunice completed her education in Radiography at FTCC and promptly commenced her career as a radiologic technologist, serving the local community.
Over her 13-year tenure at Cape Fear Valley Health System, Eunice held various pivotal roles, including Staff Technologist, Certified Clinical Evaluator/Instructor for the Radiography Program, Lead Technologist, and Supervisor of Diagnostic Radiology. She brings a wealth of practical experience and expertise to her role.
Continuing her pursuit of knowledge, Eunice earned a Bachelor of Health Science from Campbell University in 2004 and a Master of Science in Instructional Technology from East Carolina University in 2014. She remains committed to professional development, having acquired multiple certifications from the Association of College and University Educators offered by the college.
In 2010, Eunice transitioned to a career in education at FTCC, where she serves as a full-time Radiography instructor. Additionally, she plays a crucial role in the Center for Faculty Development, contributing her expertise as an instructional designer.
Through her multifaceted experiences and dedication to education, Eunice continues to inspire and empower students and faculty alike, enriching the learning community at FTCC and beyond.

CFD Fellow/Educational Evaluation/Standards
English Instructor
CUH 388
(910) 678-9775
isenhouj@faytechcc.edu
John Isenhour, an esteemed faculty fellow at Fayetteville Technical Community College’s Center for Faculty Development, brings a wealth of experience spanning more than two decades to his vital role. Armed with a Bachelor’s degree from UNCP and a Master’s degree from UNCG, John has been an integral member of the English faculty since 2003.
John’s dedication extends to a multifaceted set of responsibilities within the Center for Faculty Development. He excels in faculty mentoring, providing invaluable guidance and support to colleagues on their professional journey. Moreover, he spearheads vibrant communities of practice focused on best practices in teaching and learning, online learning and technology, assessment and evaluation, leadership development, and student success.
With the understanding that quality is gauged through clear expectations and evaluation, John ensures that the initiatives he leads drive continuous improvement. His passion for facilitating the seamless integration of new faculty into their instructional roles and harnessing cutting-edge educational technology to enrich the learning experience underscores his commitment to fostering excellence in education.
John’s contributions not only benefit his colleagues but also elevate the institution, solidifying his status as a valuable asset to the academic community.

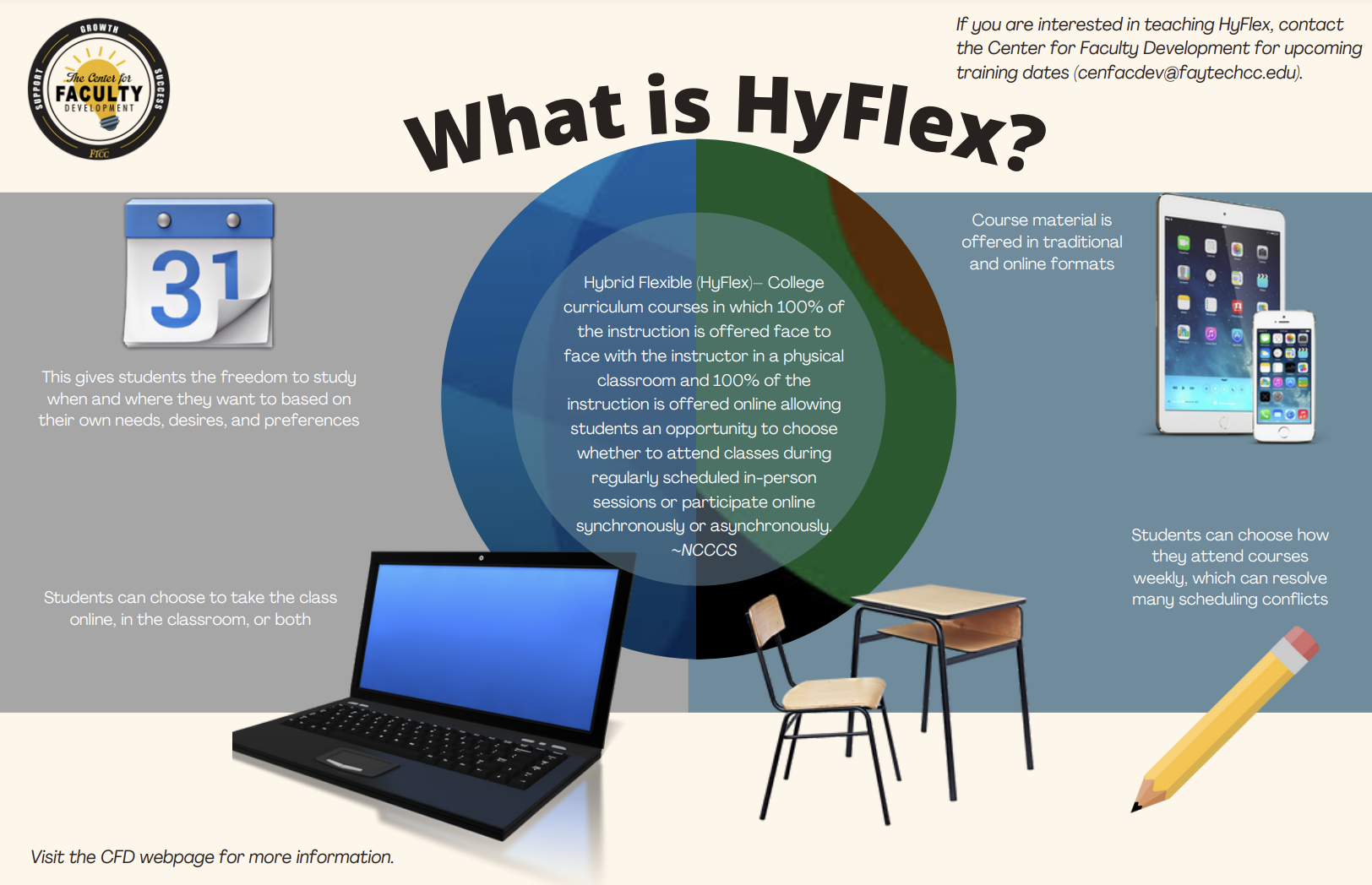
CFD Fellow/HyFlex
Criminal Justice Instructor
HOS 633
(910) 678-0045
osbornje@faytechcc.edu
Jennifer Osborn, a distinguished Faculty Fellow at the Center for Faculty Development, Fayetteville Technical Community College, brings a wealth of experience and a strong commitment to education.
With over 17 years of dedicated service as a highly decorated police officer, Jennifer has consistently demonstrated unwavering dedication to public safety. She is a recipient of the prestigious Hometown Hero Award, presented by the Governor of North Carolina, for two consecutive years, highlighting her extraordinary achievements in saving lives and facilitating educational milestones for others.
Beyond her professional accomplishments, Jennifer is a devoted mother of two and the spouse of a current police officer. Her passion for lifelong learning is evident in her pursuit of a Ph.D. and the successful completion of her Executive Criminal Justice Certificate.
Jennifer’s diverse background, coupled with her unwavering commitment to education, positions her as a valuable asset to the Center for Faculty Development. She eagerly anticipates the opportunity to contribute to a collaborative and enriched academic environment, where her expertise will empower faculty and foster a culture of excellence

CFD Fellow/SIBME
Program Coordinator-Elementary Education Residency Licensure
Education Instructor
CUH 302
(910) 678-9790
cravenh@faytechcc.edu
Heather Craven, a dedicated faculty fellow at Fayetteville Technical Community College’s Center for Faculty Development, brings a wealth of experience and expertise to her role. Currently serving as a full-time instructor in the Education Department, Heather also holds the esteemed position of Residency Licensure Certificate Program Director for the innovative program in Elementary Education. Her commitment to education spans over 16 years, during which she has excelled in various roles such as mentor, tutor, teacher, Instructional Coach, and Assistant Principal.
Heather’s academic credentials include a Bachelor of Science in Elementary Education and a Master of Arts in Executive Leadership, accompanied by a K-12 Administrator’s License. Her wealth of knowledge and extensive background in education make her a valuable addition to the team.
In her capacity as our SIBME Ambassador, Heather is enthusiastic about using her expertise to enhance faculty development and promote excellence in teaching practices at FTCC. This platform and tool are designed to support video-based coaching, mentoring, and professional development across various educational settings, including K-12 schools, colleges, and universities. SIBME empowers educators to record classroom or instructional sessions and share them with mentors, coaches, or colleagues for feedback and reflection. With SIBME, Heather aims to assist educators in improving their teaching practices, enhancing their professional development, and ultimately fostering effective teaching and learning experiences.

CFD Fellow/Instructional Design
Communications Instructor
LRC 122
(910) 486-7312
mitchelb@faytechcc.edu
Mrs. Brenda Mitchell, M.Ed., is a distinguished full-time Communications instructor at Fayetteville Technical Community College, where her dedication to education shines. In addition to her role as an educator, Brenda serves as a Faculty Fellow in the Center for Faculty Development, contributing her exceptional skills as an Instructional Designer.
With an impressive 15-year tenure in education, Brenda’s career has been defined by an unwavering passion for both students and faculty members. Her primary mission is to instill confidence, not only in her students but also in the faculty she collaborates with.
As an instructional designer, Brenda excels in empowering educators by implementing effective strategies and innovative techniques. Her responsibilities encompass curriculum design and enhancement, the seamless integration of technology to optimize learning experiences, and the provision of invaluable coaching to fellow faculty members. Brenda’s tireless efforts are dedicated to enhancing the overall educational journey, promoting excellence in teaching and learning, and equipping instructors with the skills and tools they need to excel in today’s dynamic educational landscape.
Fayetteville Technical Community College confers the OSHA 30-Hour General Industry microcredential recognizing individuals who master workplace safety and OSHA standards. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.

Click the icon for additional information
Fayetteville Technical Community College confers the OSHA 30-Hour Construction microcredential recognizing individuals who master workplace safety and OSHA standards. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.

Click the icon for additional information
Fayetteville Technical Community College confers the OSHA 10-Hour General Industry microcredential to individuals who master specific safety and health topics required to satisfy both federal OSHA requirements and North Carolina’s state-specific rules. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.

Click the icon for additional information
Fayetteville Technical Community College confers the OSHA 10-Hour Construction microcredential to individuals who master specific safety and health topics required to satisfy both federal OSHA requirements and North Carolina’s state-specific rules. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu

Click the icon for additional information
Fayetteville Technical Community College’s Continuing Education Program, in collaboration with the Industrial Systems Technology Program, offers the ‘Personal Safety’ microcredential. Earners of this badge completed the 5 hours of OSHA-10 training relevant to personal safety. This microcredential is one of a two-part series within the “Industrial Safety” macrocredential pathway. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.
Fayetteville Technical Community College’s Supply Chain Management Programs offer a Verified Forklift Operator microcredential endorsing earners as proficient in safe and efficient forklift operations. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.

Click the icon for additional information
Fayetteville Technical Community College’s Transition Tech Program offers a microcredential signifying the earner’s fundamental understanding of Lean Six Sigma methodologies (Yellow Belt). If you are interested in earning this badge, please contact:
Pendy Eldridge, Transition Tech Recruiter.

Click the icon for additional information
Fayetteville Technical Community College’s Transition Tech Program offers a microcredential signifying the earner’s fundamental understanding of Lean Six Sigma methodologies (Green Belt). If you are interested in earning this badge, please contact:
Pendy Eldridge, Transition Tech Recruiter.
Click the icon for additional information
Fayetteville Technical Community College’s Continuing Education Programs, in collaboration with the Industrial Systems Technology Program, offers the ‘Industrial Hazards’ microcredential. Earners of this badge completed the 5 hours of OSHA-10 training relevant to industrial hazards. This microcredential is one of a two-part series within the “Industrial Safety” Macrocredential pathway. If you are interested in earning this badge, please contact:
FTCC Corporate & Continuing Education: Corporate & Industry Training.
industrytraining@faytechcc.edu.
Fayetteville Technical Community College’s Medical Technology Program offers the microcredential in Diagnostic Microbiology. If you are interested in earning this badge, please contact:
Henock Haile, Department Chair.

Click the icon for additional information
Fayetteville Technical Community College’s Medical Technology Program offers the microcredential in Diagnostic Hematology. If you are interested in earning this badge, please contact:
Henock Haile, Department Chair.
Click the icon for additional information
Fayetteville Technical Community College’s Medical Technology Program offers the microcredential in Diagnostic Clinical Chemistry. If you are interested in earning this badge, please contact:
Henock Haile, Department Chair.
Click the icon for additional information
Fayetteville Technical Community College’s offers a microcredential signifying the earner has successfully completed comprehensive training in Cardiopulmonary Resuscitation (CPR). If you are interested in earning this badge, please contact:
Corporate & Continuing Education: Emergency Services.
Click the icon for additional information
Fayetteville Technical Community College’s IT/Systems Security & Analysis Program offers the Cybersecurity Specialist microcredential, based on SEC-110, ‘Security Concepts’. If you are interested in earning this badge, please contact:
Rhiannon Holley, Department Chair.

Click the icon for additional information
